L4/5 or L5/S1 Disc Herniation — Can You Recover Without Surgery?
You've had the scan. You've read the report. And now you're sitting with words like "disc herniation,""nerve compression," or "significant canal narrowing" and not much else. And for most people (who don’t work in the medical field), the report could create a lot of anxiety surrounding your future!
If you're an active adult in London trying to figure out what this actually means for your training, your work, and your life, this post is for you.
The honest answer? Most people with L4/5 or L5/S1 disc herniations recover without surgery. A 2026 systematic review and meta-analysis of nearly 5,000 patients found that while surgery provides faster short-term relief, conservative management achieves equivalent outcomes beyond two years (Journal of Musculoskeletal Surgery and Research, 2026).
As a Specialist Spinal Physiotherapist in London, one of the most impactful things I can do in the initial session is give you what most people never receive
a clear explanation of what's actually happening
a realistic timeframe for recovery
structured roadmap from where you are now back to full performance.
You might not be sitting in front of me just yet, but consider this post my way of sharing exactly that, so you can start feeling more confident that conservative recovery is not just possible, but likely.
What Is a Lumbar Disc, and What Happens When It Herniates?
Your lumbar spine (lower back) is made up of five vertebrae, L1 through to L5. Between each vertebra sits an intervertebral disc, which has a gel-like centre (the nucleus pulposus) surrounded by a tough outer ring (the annulus fibrosus).
This video shows the lumbar spine anatomy. The discs are represented in yellow, and sit in between two vertebrae.
These discs absorb load, distribute force, and allow the spine to move. They are essential and robust structures, not flimsy, fragile things.
A disc herniation occurs when the nucleus pushes through a weakness or tear in the outer ring — typically towards the back or side, where the spinal nerves run. The disc material can then compress or irritate a nerve root, which then could create symptoms typical of ‘sciatica’.
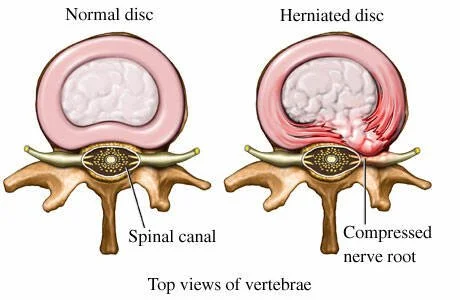
Material from the nucleous pulposus breaks through the disc barrier and enters the spinal canal, compressing the nerve roots (leading to ‘sciatica’)
The most commonly affected levels?
The two most commonly affected levels are:
L4/5 — where the L4 or L5 nerve root can be affected
L5/S1 — where the L5 or S1 nerve root is most commonly involved
These levels sit at the base of the lumbar spine, and have a bigger role in absorbing your weight/load/impact. Which is precisely why they're the most common sites of disc injury.
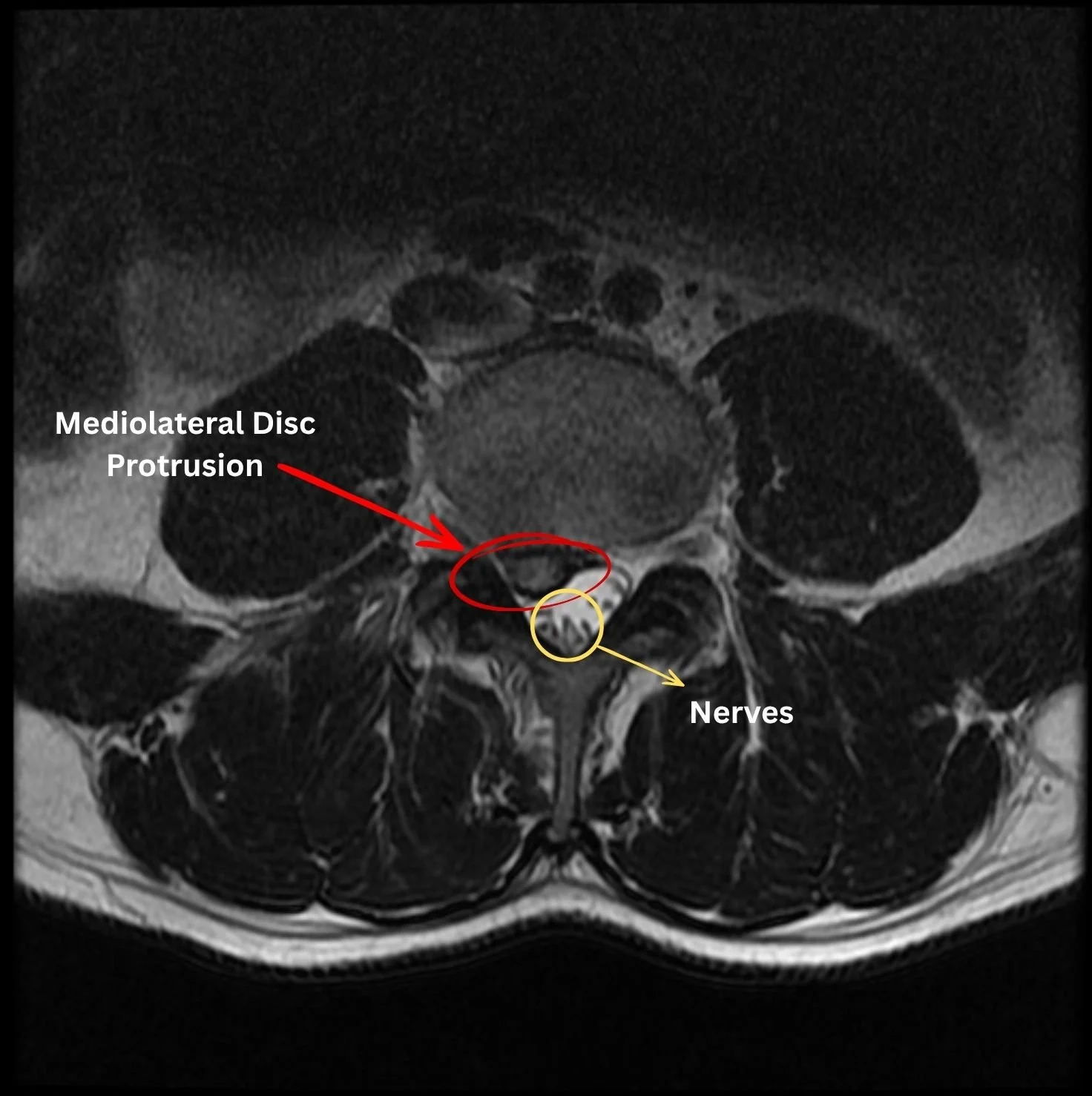
MRI of a mediolateral lumbar disc protrusion showing compression of the spinal nerves in the spinal canal.
The Spectrum of Disc Pathology
There are many ‘types’ of disc injuries, all of which may (or may not) contribute to your symptoms:
Disc bulge — generalised, symmetrical outward expansion of the disc.
Disc protrusion — focal herniation where the base is wider than the displaced portion.
Disc extrusion — displaced material where the base is narrower than the herniation.
Disc sequestration — a fragment has broken free entirely.
The words on your report can sound alarming. But the severity of your symptoms and the clinical findings from a comprehensive assessment is what guides management. We never treat the scan, we treat the person in front of us (YOU!).
Many disc extrusions and sequestrations do very well conservatively as the body’s natural healing mechanism seems to be able to resorb extrusions and sequestrations (however, this does depend on patient symptoms and the presence of neurological signs).
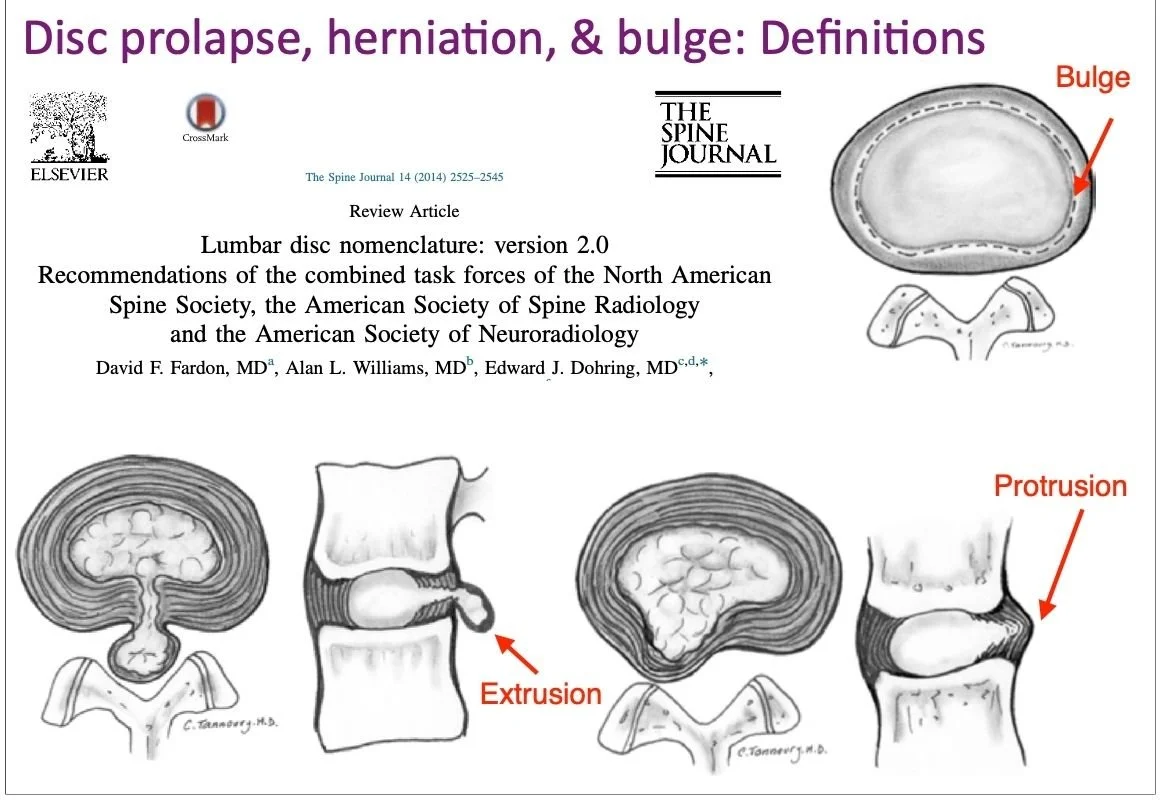
Image depicting the different types of disc pathology.
Why Your MRI Report Can Be Misleading
This is one of the most important things I tell my clients.
MRI scans are extraordinarily sensitive. They pick up structural changes that have often been present for years — completely silently.
A landmark study published in the New England Journal of Medicine found that over 50% of people with no back pain at all showed disc bulges or herniations on MRI. By the age of 50, degenerative disc changes are present on imaging in the vast majority of asymptomatic adults.
This does not mean your pain isn't real. It absolutely is.
What it means is that the disc change on your scan is not automatically the villain. Understanding the relationship between what we see on imaging and what you're actually experiencing, that's where clinical assessment becomes essential.
Our role as Specialist Physiotherapists in Spinal conditions is to use MRI reports to ADD to our clinical confidence, not to be used in isolation to treat you. The MRI report doesn’t show meaningful things like load tolerance, movement quality, neural sensitivity, or why your symptoms came on when they did.
What Symptoms Actually Tell Us
Disc herniations at L4/5 and L5/S1 typically produce symptoms in a recognisable pattern, depending on which nerve root is compressed.
L4/5 Disc Herniation — L4 or L5 Nerve Root Involvement
Pain, numbness, or pins and needles into the outer thigh, shin, or top of the foot
Weakness in ankle dorsiflexion (difficulty lifting the foot — sometimes called "foot drop" in severe cases)
Reduced sensation over the outer shin or top of the foot
L5/S1 Disc Herniation — L5 or S1 Nerve Root Involvement
Pain or altered sensation into the calf, heel, or outer edge of the foot
Weakness in calf raises (ankle plantarflexion)
Reduced or absent Achilles reflex (tested clinically)
The specific distribution of your symptoms, where exactly the pain travels, what makes it worse, and what relieves it, gives us far more information than the scan alone.
Here’s the other nuanced part about Sciatica (or what you think might be sciatica).
Not all leg pain is nerve pain, and not all nerve pain means structural compression. Neural sensitivity can perpetuate symptoms long after the mechanical cause has resolved. This is a crucial distinction in deciding how to manage you.
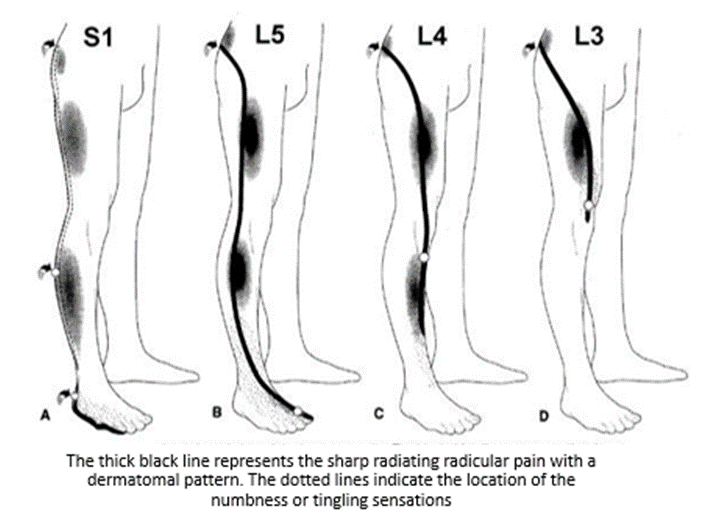
Typical patterns of pain in ‘Sciatica’ that affects different levels. *Important* - not everyone will follow this textbook presentation!
When is Surgery Necessary for Disc Herniations?
I want to be clear: there are (rare) circumstances where surgery is the right decision, and good physiotherapy includes knowing when to refer. The cost of delaying surgery when it is indicated can be devastating!
Seek urgent medical attention if you experience:
Loss of bowel or bladder control, or numbness in the saddle area (groin, inner thighs, genitals) — this may indicate cauda equina syndrome, a surgical emergency
Rapidly progressive leg weakness — particularly if it is developing over hours to days
Severe, unrelenting pain that is not responding to any position or movement after several weeks
For the vast majority of disc herniations, however — including those causing significant sciatica — surgery is not the first or inevitable answer.
The Evidence for Conservative Management
The research on lumbar disc herniation is reassuring and consistent.
Studies tracking people with confirmed disc herniations, including those causing nerve pain, show that the majority experience significant improvement with conservative management over 6 to 12 weeks. Importantly, follow-up imaging has shown that disc herniations can and do resorb over time, particularly extruded and sequestered fragments, which provoke an immune response that gradually reduces their size.
Surgery has a role — particularly when conservative care has failed over an adequate timeframe, or when neurological deficit is severe or progressive. But the evidence consistently shows that outcomes at 1 to 2 years are similar between surgical and non-surgical management in most cases. The key difference is speed: surgery can get you there faster. But it carries risks that conservative management does not.
For most active adults, a well-structured rehabilitation programme gives excellent outcomes.

Spinal rehabilitation exercise: Bird Dog, designed to target deep lumbar extensor muscles and abdominal muscles to rebuild stability in the lower back.
How I Approach L4/5 and L5/S1 Disc Herniation injuries at Physiologic London
No two disc herniations are the same, and no two people are the same. My approach begins with understanding yours specifically.
Phase 1: Comprehensive Assessment
Before any treatment, here are some important points I need to understand:
The history of your condition. Was there a gradual increase in symptoms or did they suddenly come on with a clear mechanism?
What is the nature, distribution, and behaviour of your symptoms?
What aggravates and what relieves (directional preference is highly informative)
Your neurological status (strength, sensation, reflexes)
Your movement patterns and how load is being distributed through your spine
Your goals — whether that's returning to the gym, marathon training, or simply getting through a day at your desk
Here I am assessing the Achilles reflex, and it clearly shows an ‘Absent’ achilles reflex on the left leg (top leg) indicating a high likelihood of an impinged L5/S1 nerve root.
The clinical assessment tells me far more than the MRI report alone. Together, they build the full picture.
Phase 2: Pain Relief and Neural Calming
If someone has presented to me in the acute phase (early phase), then the priority is:
Reducing pain and neural sensitivity.
Identifying positions and movements that centralise or reduce symptoms (directional preference)
Restoring basic confidence with movement
We know that the first 10-14 days are typically going to be quite painful for our clients as they navigate through the inflammatory phase of their injury, so helping manage their pain early on is key to setting them up for a successful recovery. Manual therapy, dry needling, and soft tissue work all have a role here, not as passive treatments in isolation, but as tools that enable active rehabilitation to begin.
Dry needling to the lower back for pain modulation.
Phase 3: Restoring Movement and Motor Control
As symptoms settle, we address the patterns that placed excess load on the disc in the first place.
Common contributing factors I see at L4/5 and L5/S1 include:
Poor lumbopelvic control — inability to dissociate hip from lumbar movement
Hip mobility restrictions — When hip mobility is impaired, it may force a compensation strategy where the lumbar spine takes on more load
Global flexion loading patterns — repeated lumbar flexion under load (common in desk workers and certain gym movements) that exceeds the disc's tolerance
Inadequate posterior chain loading — apart from the ‘weak glutes and hamstrings’, most tend to either forget, or avoid, loading the spinal extensors (erector spinae). It is absolutely crucial to target these muscles as they have been proven to develop fatty infiltrate over time especially in disc herniation presentations.
Addressing these is not about treating the disc directly. It is about changing the mechanical environment the disc is influenced by, in search of longer term solutions.
Rehab exercise for disc herniation: Single leg isometric glute bridge for posterior chain activation and strength
Phase 4: Progressive Spinal Loading
This is where most other approaches fall short — and where I believe the biggest difference is made.
The spine needs to be loaded. Progressive, graduated loading is what drives tissue adaptation, reduces neural sensitivity, and builds the long-term resilience that prevents recurrence.
This means returning to deadlifts, squats, carries, and running, but doing so intelligently, in a sequenced way, based on your tolerance and response.
Avoidance builds sensitivity, and fear around movement. Progressive loading builds resilience and confidence to truly get back to feeling 100%.
Spinal Loading exercise (advanced): The trap bar deadlift is an excellent way to build spinal loading tolerance as there is less shearing forces on the spine.
The aim is not to protect the spine from the world. The aim is to prepare the spine for the demands you want to place on it.
Can You (should you) Still Train with a Disc Herniation?
Short answer is YES in most cases.
This is the question I hear most often from active adults, and most, if not all of them, are glad to hear that I usually say YES!
Training does not need to stop. In many cases, it shouldn't. Maintaining fitness, muscle mass, and cardiovascular capacity during rehabilitation is protective and helps keep you in the habit of continuing your usual gym routine.
What changes is how you train:
Acute flare-up: Modify load, range, and direction based on what centralises your symptoms. Avoid prolonged lumbar flexion under heavy load. Maintain movement in tolerable ranges. In plain english, that means that you may need to, for a short period of time, reduce the weights, don’t squat as low, and maybe replace certain movements with others that are more tolerable for you.
Sub-acute phase: Reintroduce loading patterns progressively. Bias posterior chain. Avoid repetitive end-range flexion under load. Swimming, cycling, and controlled gym work are often well-tolerated.
Rehabilitation phase: Systematically reintroduce all movements, including those that previously aggravated in a graduated way. The goal is a spine that can do everything again, not a spine that you keep in ‘neutral’ all day.
Return to Sport phase: Using Strength and Conditioning principles and working with our industry colleagues, this is when we introduce dynamic movements, plyometrics, change of direction drills etc to get you back to performing your best.
Progression from one phase to the next will be based on a combination of ‘timeframes’ AND most importantly, ‘passing objective tests’.
Internal Links for Further Reading
👉 Sharp Lower Back Pain on One Side? It Could Be a Lumbar Facet Joint Irritation
👉 Managing Spondylolisthesis: A Spinal Physiotherapist's Guide to Long-Term Relief
👉 Is a Diagnosis Crucial for Managing Spinal Conditions?
When to See a Spinal Physiotherapist in London
If you've been given an MRI report showing L4/5 or L5/S1 disc herniation and aren't sure what to do next — a thorough clinical assessment is the best place to start.
Not to confirm what the scan shows. But to understand what it means for you, your symptoms, your movement, your goals and to build a plan that reflects all of that.
If your pain has been going on for more than 6 weeks, is stopping you training, or has resulted in symptoms travelling into the leg, it is worth having a proper spinal assessment sooner rather than later.
👉 Sports & Spinal Physiotherapy in London — Learn More
About the Author
Ryan Tan Sports & Spinal Physiotherapist | Physiologic London
Ryan is a specialist Sports & Spinal Physiotherapist with over a decade of clinical experience across Australia, Hong Kong, and London. He holds a Certificate of Spinal Manual Therapy (COSMT) and is trained in Osteopathic Spinal Manipulation (OMT).
He has worked in complex pain clinic settings alongside Pain Consultants and Spinal Neurosurgeons, and currently works with some of London's leading orthopaedic spinal surgeons to deliver integrated, expert care for clients with complex spinal conditions.
At Physiologic London, Ryan specialises in helping active adults with persistent lower back pain, disc herniations, and nerve-related conditions return to training, sport, and the life they want to live — without unnecessary surgery.